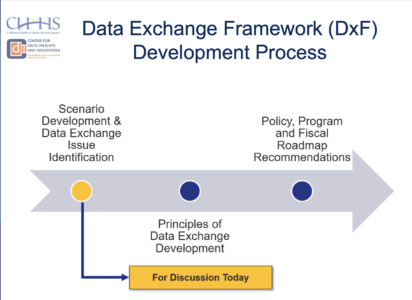
We were thrilled to watch the second meeting of the Data Exchange Framework (DxF) Stakeholder Advisory Group on October 7––a discussion that was shaped largely by example scenarios in which data exchange could be utilized. As illustrated in the slide below from the presentation, the development of these key scenarios is the first of three tentpole steps of the DxF development process:
California HHS Secretary Dr. Mark Ghaly opened the meeting with an important––and blunt––statement: “Where we are today doesn’t work. We continue to fail our communities and our populations because of the lack of consolidated information around specific individuals, populations and communities. We will continue to keep…the communities we serve front and center in these conversations. We want to build something we can all be proud of.”
As a coalition, we strongly agree with this assertion, and believe that the DxF Stakeholder Advisory Group process could go a long way towards changing the status quo––especially for the many communities in California who have extremely inequitable access to health data. COVID-19 revealed all too starkly how quickly poor health data infrastructure can turn into dire health impacts for entire communities. We continue to believe that a statewide HIE network is the only way to guarantee high-quality, accessible, and secure health data for every California patient and provider. COVID-19 made obvious the many shortcomings in California’s health data infrastructure, and the latest stage of combating the virus––the rollout of the vaccine to tens of millions of people––is the strongest mandate for statewide health data exchange.
We were pleased to see many members of the group both attest to the urgency, and the potential positive impacts on health equity in California. This dynamic became clear during discussions of the scenarios, which––as many members of the group pointed out during the meeting––were less focused on consumers than they ought to have been. As Mark Savage, Managing Director of Digital Health Policy at Savage & Savage, LLC, noted, “With one exception, the scenarios do not have any information flows with the individual at the center of care.”
As Amanda McAllister-Wallner, CA LGBTQ Health & Human Services Network Director for Health Access California noted, “It’s crucial that we put consumers at the heart of how we design the data systems. How will consumers access this data, both to update/provide info, and get information that is crucial for managing their health?”
We agree that considering the experience of the individual consumer is paramount, and believe it would be a mistake to center the discussions or scenarios around other related players too firmly. (This builds on a discussion raised in the first meeting, that the role of the patient should be front and center).
In large part, putting patients first is important because ensuring trust among the community is critical to the success of any data exchange framework. As Lori Hack, Interim Executive Director of the CA Association of Health Information Exchanges (CAHIE) said, “We have established a circle of trust in the community, where we’re sharing data from one provider to another. Some of the key components to build trust are accountability, transparent policies, helping the community to understand who the data steward is. Accountability, consent, oversight or enforcement, and finally…education and training of the stakeholders who are accessing data, to make sure they’re doing it properly.”
In the end, the second stakeholder meeting was a robust discussion on the path forward for data exchange in California, and made clear to us what we see are the 7 ingredients to a successful data exchange framework in the future:
- Data standards (e.g., USCDI v.1-2, +)
- Consent, privacy and security (e.g., HIPAA, CMIA, CalDURSA and other programs and laws)
- Infrastructure (e.g., statewide HIE network leveraging existing infrastructure)
- Funding and incentives (e.g., MITA, ARPA, other funding streams; plan and state incentives)
- Identity management for providers and patients (e.g., EMPI, ACRS)
- Governance, enforcement, and accountability mechanisms (e.g., state CHHS leadership and action)
- Patient and consumer engagement (e.g. education and other programs)
These 7 pieces, put together, will shore up community trust in the system, ensure it is well-resourced into the future, and have both the rules and technological infrastructure in place to deliver on the ambitious goals to deliver better health data––and health outcomes––for every Californian.