On September 30, we were joined in our biweekly coalition meeting by Rich Boehm, Vice President of Informatics, Operations and Provider Systems with BCBS of Michigan, and Tim Pletcher, Executive Director of Michigan Health Information Network (MiHIN) Shared Services. They shared countless valuable insights about how MiHIN came to be, its positive impacts, and how they’re aiming to improve it going forward. Their full presentation is linked here.
To begin, Tim and Rich discussed the four major steps they navigated toward building the robust MIHIN system––which are reflective of those we have identified in California as well. As the below graphic illustrates, Michigan is now firmly in stage 4, as MIHIN can support interoperability, reduce burdens, and continues to drive innovation in support of improved care outcomes for patients. California, on the other hand, at a state level, is very much still in stage one, working to engage stakeholders and develop a statewide vision for data sharing.

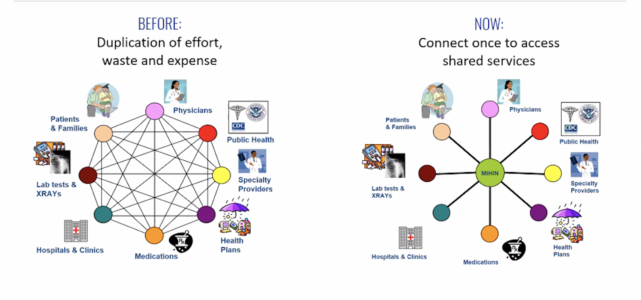
As a way of illustrating the benefits Michigan saw in developing a statewide network, Tim and Rich presented the following illustration to represent how efficient a statewide HIE network can make data sharing.
A key portion of the discussion with Rich and Tim centered on their experience regarding, and best practices surrounding, incentives. They presented the following slide highlighting their innovative and highly successful approach:

A key piece of the puzzle in building MiHIN is ensuring health plans tie financial incentives to key use cases. As Tim said, “Things don’t need to take years when you use this model. It can all happen in a year. You pay people, things can move quickly.”
Going forward, Tim said legislation could become necessary to further cement MiHIN as a data utility. Specifically, Tim wants the Michigan State Legislature to pass legislation supporting a true public health utility. As he said, “COVID showed us we need to think bigger than EHR. The HIE model is not sustainable––it doesn’t make room for community health organizations that have played a key role.”
He continued, “We need to involve corrections, social workers, foster care and other organizations that meet the patient where they are.”
Rich and Tim presented a compelling roadmap towards building a statewide HIE network––because while Michigan and California are different in many ways, certain best practices are universally applicable. As Tim said in closing, “Put money in the right spot and give people the right incentives, and you can get stuff done in just a matter of months.”